Something is clearly off (concerning) in the CDC data regarding Moderna’s mRNA-1273 vaccine. Considering the CDC just revised its count of child deaths due to an “algorithm” error my last statement may not strike you as odd, but hear me out. Especially since Moderna is seeking EUA approval for its vaccine among children younger than six, with relatively shoddy outcomes. To be sure a plant based diet is more effective at preventing COVID severity and therefore likely hospitalization and death, at least for adults, with less risks.
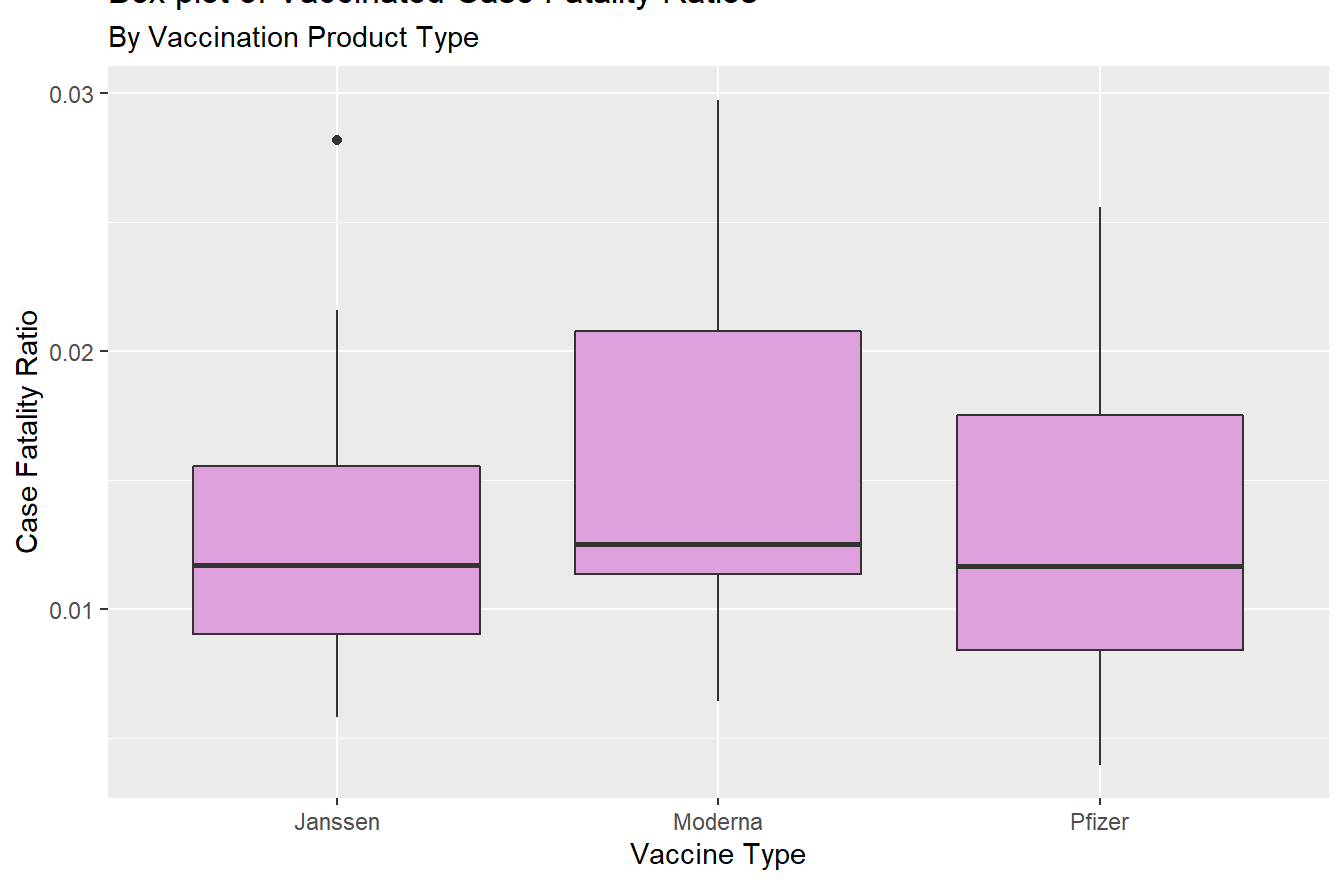
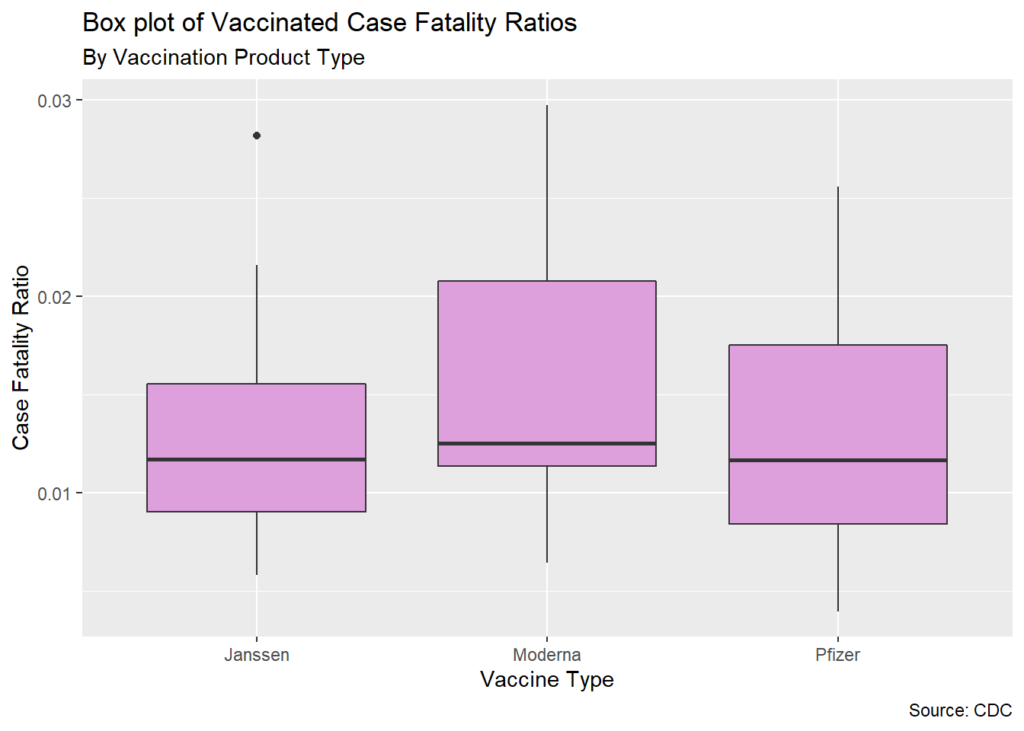
Case Fatality Ratios – a measure of how likely someone is to die after infection, in this case from COVID-19 and also in this case implied from multiple signals in the CDC data – are significantly higher for recipients of Moderna’s vaccine than for either Janssen (J&J) or Pfizer recipients. This means that although all the vaccines offer mostly robust protection against death or hospitalization from a SARS-COV-2 infection, there’s reason to believe that those who took Moderna are more likely to die after infection than their vaccinated peers.
Case Fatality Ratios or CFRs matter because death rates don’t control for methods for evading an infection that may correlate with the probability of getting vaccinated and mask (dark pun) the true effectiveness of the pharmaceutical intervention. This in part explains why mortality rates were nine times higher for the unvaccinated in 2021 but CFRs were barely twice as high: people who were vaccinated were also less likely to be infected, and not necessarily because of protection from the intervention. Presumably though infection is necessary to be a candidate for death, so it makes the most sense to at least exclude people without verified infections. This makes CFRs a stronger, even if not the strongest, measure of vaccine effectiveness.
As far as I know no one else has reported on the measurable difference between Moderna’s CFR and the other vaccine types.
This still isn’t a perfect measure at least because of the confounding effects of asymptomatic spread. A lot of us were exposed and infected with few to no symptoms. So we’re certainly underestimating denominator in CFRs (Fatal Cases / Infected Cases). In late December – peak 2021 infection rates – about 1% of unvaccinated and 0.4% of vaccinated people were reporting a cases weekly. This was likely a mix of people caught in mandatory testing nets and those sick enough to seek testing. As such our CFR is really a CFR of that population: people forced to get testing.
Keep that in mind: all of these rates are likely bigger than they would be with perfect information. And they’re already remarkably small.
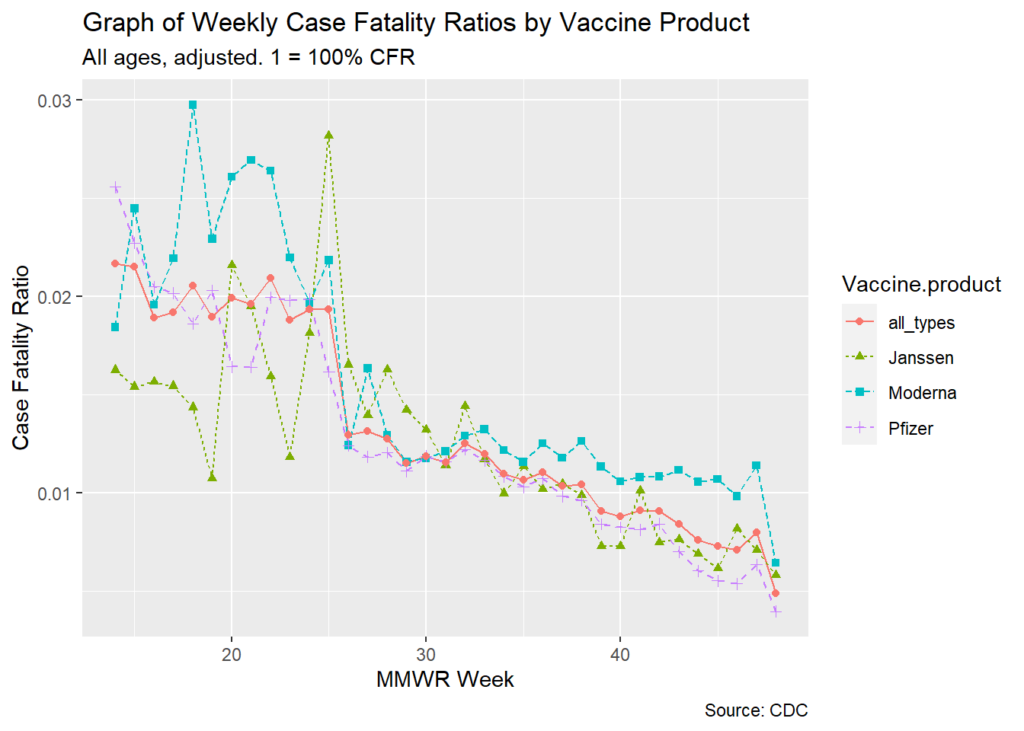
Moderna’s CFRs have been statistically higher than the other two vaccines throughout 2021. From the very beginning. All of this would be less concerning if the variance was only observed in a few sporadic months, or just at the beginning when the vaccine was only available selectively, but no: this is all year. Virtually every week. This patterns suggests to me a systemic issue particular to the Moderna vaccine or its recipients.
I suggest three potential explanation for this phenomenon in the data, in an order I think reflects the hear-hoofs-think-horses-not-zebras mentality.
1) Moderna’s Recipients Are Less Likely To Test Positive, Artificially Suppressing The CFR Denominator
The least sensational even if not the most likely explanation is that Moderna recipients are showing up as COVID-19 positive less often than other vaccine types, inflating the ratio of lethal cases to positive cases. This could be reflective of interactions with testing self-selection: if Moderna reduces the severity of COVID-19 symptoms across the distribution particularly well then fewer recipients may select to test and those who do may be more symptomatic than the average vaccine recipient. It also isn’t necessary for recipients to be less likely to have symptomatic illness. Perhaps there was a systemic issue with processing tests from Moderna recipients.
I could take this explanation more seriously if there was better supporting evidence. One would imagine in a world determined to portray the vaccines in the best light possible it would have been a massive oversight for researchers, public health officials, and major media outlets to ignore solid evidence that even one of the vaccines was confidently protecting people from infection. So much was the original messaging before real world data on relatively rampant breakthroughs tossed away that pipe dream. Although there have been suggestions that Moderna was more resilient against breakthroughs I don’t think that is enough to confidently explain a higher CFR.
2) Moderna’s Recipients Are Disproportionately Older Than Other Vaccine Recipients
It’s possible that Moderna is being pushed more than other vaccine types in senior centers and hospices, and the CDC data supports that vaccine recipients still suffer from an age-based risk gradient: COVID illness is more fatal with age. In this case Moderna would be carrying an inordinate part of the burden for inoculating the elderly – and showing it in its case fatality rates.
The CDC does provide vaccination status by age, but not by age and vaccine type to my knowledge – surprise! I’m sure it’s for the same reason that this post exists that the CDC doesn’t provide vaccine type data by age and infection or fatality. Imagine if I could identify CFR inconsistencies between age groups by vaccination status? Or understand whether vaccine effectiveness was robust to age-segmentation by vaccine type? In any case the CDC seemingly doesn’t want us to know how vaccine types are being distributed – or their effectiveness – by age, so there’s no way to completely rule out this possibility.
For what it’s worth at least one study funded by the CDC to analyze VAERs and v-safe data found that between December 14th 2020 and June 14th 2021 the median age of Moderna recipients (56) was 6 years older than Pfizer.
3) Moderna’s Heart Muscle Tissue Inflammation and Related Complications Are Reducing Case Survival Odds
Admittedly this is the most sensational explanation, but also the most reliant upon peer reviewed studies. It also doesn’t require me to speculate about hypothetical issues within the data and focus on how a documented issue could be hypothetically driving outcomes seen in the data. The difference is critical: I’m speculating that the previously discussed data and vaccine distribution issues exist, whereas the issue here is known – whether it’s driving higher CFRs is at least a matter of mechanism (being mindful that without experimentation we can’t reasonably determine causality).
The issue is that myocarditis and pericarditis – inflammation of the heart and tissue around the heart – are common serious adverse reactions to the mRNA-type vaccines. It should be said that most adverse reactions seem to be mild – headaches, local area pain and swelling – and relatively infrequent (based on VAERS reports in the hundreds of thousands vs hundreds of millions of doses). But the CDC study I cited in the last section also found that 8.9% of reported adverse reactions ranged from serious to lethal (for Moderna specifically this figure is 7.3%). Cardiovascular related adverse reactions, including coagulopathy, stroke, and myopericarditis featured prominently in the adverse events of special interest in this study.
Interestingly a wider-window analysis in the Journal of Personalized Medicine of VAERs finds higher rates of myocarditis and pericarditis than the CDC’s study: over 5 incidents per million doses vs over 3. But this rate varies by age, reaching nearly 21 incidents per million doses for those between 12 and 17 years old. Remember how I brought up vaccination risks in the first paragraph of this post? This is particularly relevant for young people who face outsized risks on some measures.
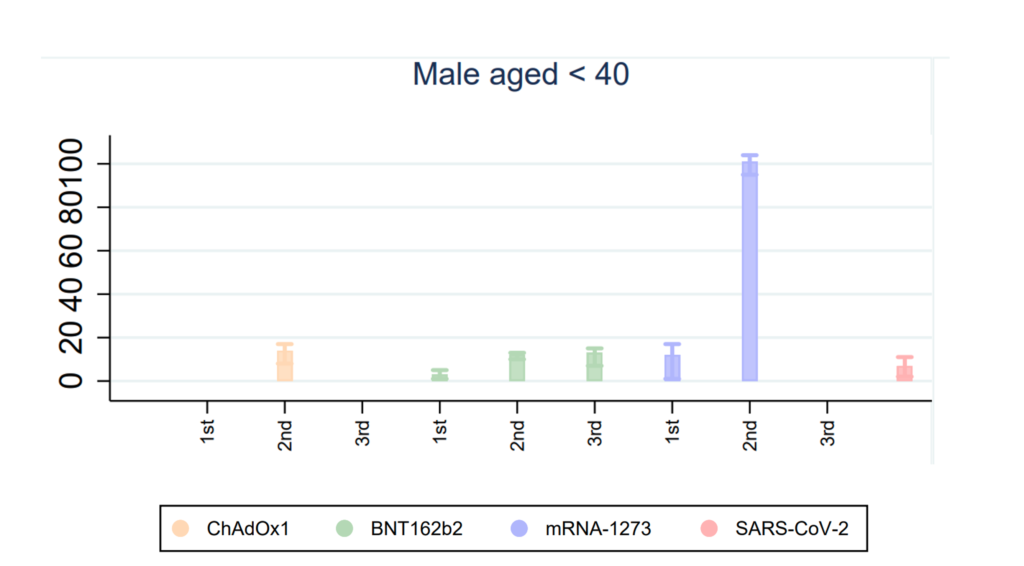
The rate also varies by vaccine type, and notably the JPM study finds higher event rates from the second dose of Pfizer than Moderna. That somewhat contradicts a Nature Medicine paper published on December 14th finding higher myocarditis events from Moderna’s second dose versus not only Pfizer’s second dose but also viral infection, for recipients under 40 years old. The risk differences between vaccine types and infection is even more stark for Moderna recipients who were young men. Notably a critical difference between the two mRNA vaccines is that Modern’s regular adult dose is over three times larger and its boosters are almost twice as large. Some have speculated that dose timing and size might be a relevant factor.
Now the mechanism: cytokine storm inflammation has been generally accepted as the cause of most COVID-related deaths. It’s been one of the earliest and most consistent parts of the scientific understanding around infection from the virus. Is it possible that the causes of post-vaccination heart tissue inflammation in Moderna recipients can happen in gradients of intensity, leading to clinically undiagnosed cases of myocarditis and pericarditis, perhaps among men over 40 and even women? Would those causes interact with a post-vaccination infection to increase the likelihood of a fatal cytokine storm among that fraction of recipients already susceptible to fatal storms? Consider that it would take precisely a small subset of recipients experiencing this to create CFR signals that would seem elevated compared to other vaccine types but still significantly lower than unvaccinated CFRs.
Ultimately this post of evidence-based speculation is why we need longitudinal, randomized control trials with anonymized publicly accessible data for these interventions. Recipients should understand how their personal health factors may adversely interact with the vaccines, and the only way to understand that is to soberly interrogate data inconsistencies like this one. Instead of discouraging public data transparency and pushing forward a wildly unserious and unscientific “safe and effective” message more appropriate in an Orwellian chapter, it would be nice to see a public health response more willing to acknowledge the realities, risks, and rewards of these interventions while treating us like adults.